Procedures
TMJ Disorders & Facial Pain
Comprehensive evaluation and stepwise management of temporomandibular joint disorders.

Understanding TMJ disorders
The temporomandibular joints (TMJs) connect the lower jaw to the skull and play a critical role in speaking, chewing, and facial movement. Disorders of the TMJ may cause pain, clicking or popping, limited jaw motion, headaches, or facial discomfort.
TMJ vs. TMD — What’s the Difference?
The terms TMJ and TMD are often used interchangeably, but they are not the same.
TMJ refers to the temporomandibular joint itself — the paired joints that connect the lower jaw (mandible) to the skull. TMD, or temporomandibular disorder, is the broader term for conditions affecting the joint, the surrounding muscles and ligaments, and the way the teeth come together.
In other words, TMJ is the anatomy; TMD is the diagnosis. Symptoms may include jaw pain, muscle fatigue, headaches, clicking or popping, limited opening, or facial discomfort.
Evaluation
TMJ-related symptoms can have multiple contributing factors. Evaluation may include a detailed clinical examination, review of dental and medical history, and advanced imaging when indicated.
Occlusal appliance therapy (more than a “bite guard”)
Occlusal appliances are commonly referred to as “bite guards,” but properly designed TMJ appliances are far more than simple night guards.
When indicated, we work closely with a patient’s restorative dentist to design an appliance that helps reduce joint loading, relax overactive muscles, and support healthier jaw function.
Unlike over-the-counter or generic appliances, these devices are custom-fabricated and prescribed as part of a coordinated treatment plan. Appliance selection, design, and adjustment are critical — and an ill-fitting appliance can worsen symptoms rather than relieve them.
This collaborative approach allows us to address both joint health and dental factors that may contribute to TMJ disorders.
Conservative therapy for TMJ pain and muscle spasm
Most TMJ disorders improve with non-surgical treatment. Initial management focuses on reducing inflammation, calming muscle spasm, and allowing the joint to rest and recover.
Common conservative therapies include:
- Activity modification and jaw rest
- Short-term anti-inflammatory or muscle-relaxant medications when appropriate
- Targeted physical therapy
- Occlusal appliance therapy
Soft diet and acute symptom management
During flare-ups of TMJ pain or muscle spasm, a temporary soft diet can significantly reduce strain on the joint and muscles.
- Avoid hard, chewy, or crunchy foods
- Avoid gum chewing and excessive jaw opening
- Cut food into small pieces
- Use moist heat or ice as directed
These measures are often combined with short-term medication and therapy to help control acute symptoms while longer-term treatment takes effect.
- Conservative Therapy for TMJ Pain & Muscle Spasm (PDF)
- TMJ Arthrocentesis Recovery Guide (PDF)
- TMJ Surgery Recovery & Diet Guide (PDF)
- Jaw locking, sudden changes in opening, or the jaw “getting stuck”
- Persistent pain or spasm that isn’t improving with conservative care
- Progressive limitation in opening, bite changes, or concern for joint arthritis/degeneration
Surgical options
If your evaluation suggests a joint‑specific problem (for example: inflammation within the joint, disc‑related dysfunction, or degenerative change), procedural or surgical treatment may be the most direct path to relief. We take a stepwise approach — starting with the least invasive option that matches your diagnosis, then escalating when it’s clinically appropriate.
Arthrocentesis (joint lavage)
Arthrocentesis is a minimally invasive procedure where the TMJ is gently irrigated (lavaged) through small needles to help reduce inflammation and improve jaw motion. It’s often considered when symptoms persist despite conservative care or when opening becomes limited (a “closed‑lock” pattern).
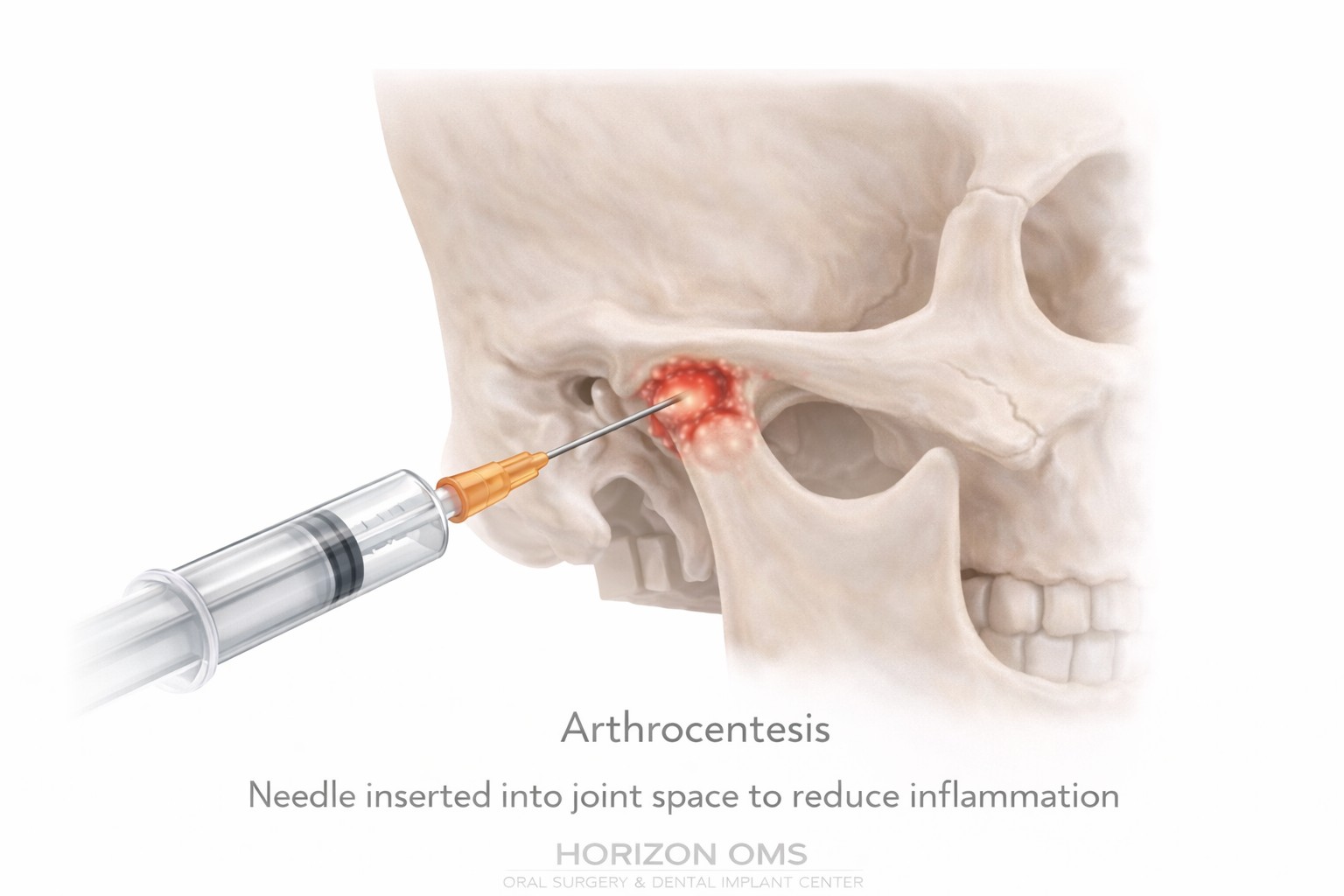
- Goals: reduce joint inflammation, flush inflammatory byproducts, and improve mobility
- Potential benefits: decreased pain, fewer flare‑ups, and improved opening/function in appropriate candidates
- How it’s done: performed with local anesthesia and, when desired, IV sedation for comfort
Adjuncts: In select cases, we may discuss intra‑articular biologics such as injectable PRF (i‑PRF) as an optional addition to help support healing and reduce inflammation. This is individualized and depends on your diagnosis and goals.
Imaging may include panoramic/CBCT to evaluate bony anatomy. In select cases, an MRI may be obtained before or after treatment to evaluate the disc and surrounding soft tissues — especially when symptoms are complex, persistent, or when surgical planning is being considered.
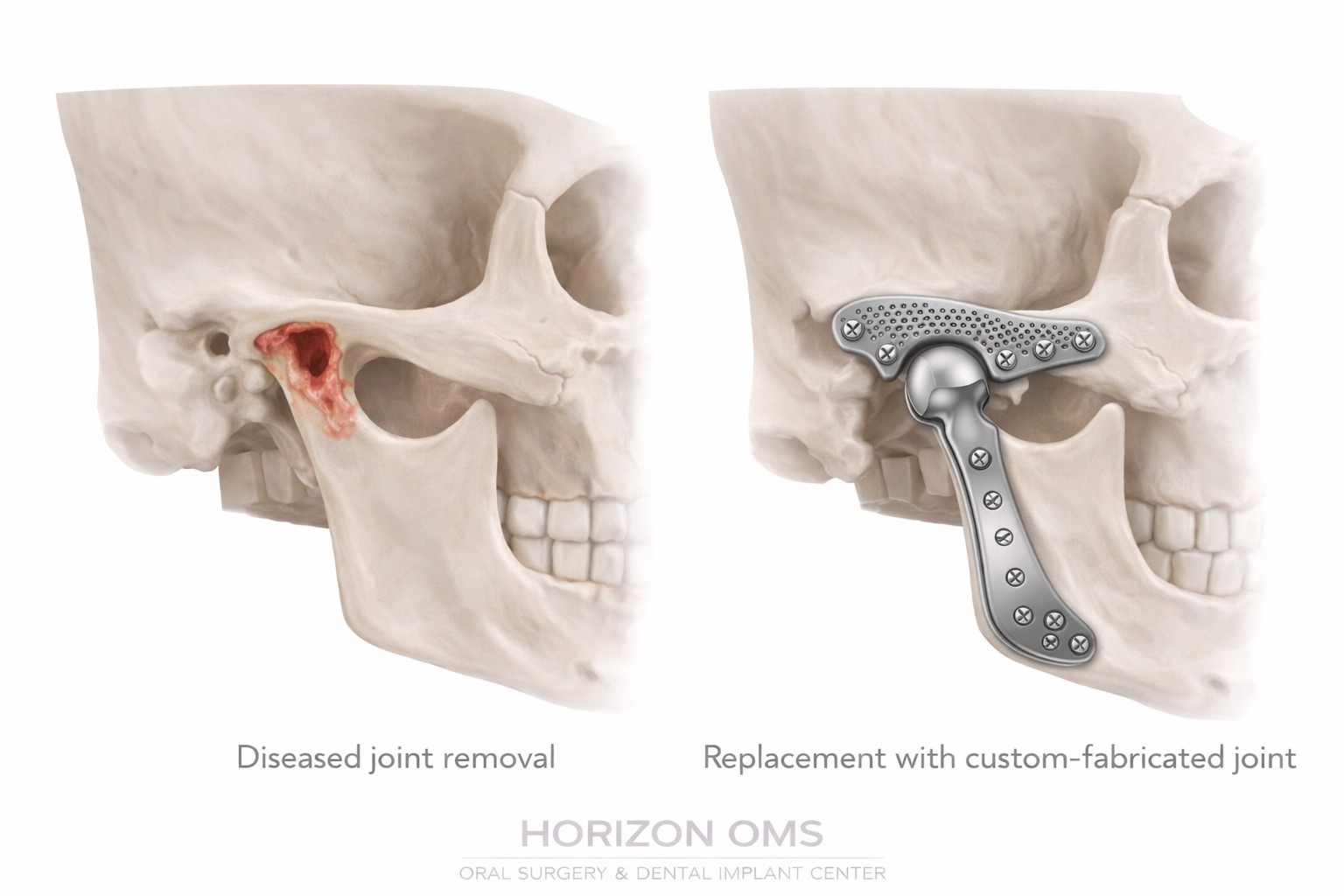
When the disc or joint is not salvageable
For advanced arthritis/degenerative disease, severe joint damage, ankylosis, or failed prior joint surgery — when the disc and joint surfaces cannot be predictably restored — we may discuss custom TMJ joint replacement.
Custom TMJ joint replacement
Custom‑fabricated TMJ prostheses are designed from your 3D imaging to match your anatomy. The goal is to restore stable joint function, improve opening, and reduce pain for patients who are appropriate surgical candidates.
- Hospital‑based surgery: performed under general anesthesia in a hospital setting, typically with an overnight (23–24 hour) stay for monitoring
- Small incisions: commonly a preauricular incision (in front of the ear) and a submandibular incision (along the jawline/neck) to access the joint and jaw
- Recovery: structured follow‑up and jaw‑function rehabilitation to support long‑term outcomes
Outcomes & success rates (what the literature shows)
In published studies and pooled analyses, total TMJ replacement is consistently associated with meaningful improvements in pain and function for properly selected patients. A 2024 meta‑analysis reported an overall implant survival around 97% (with low certainty of evidence across studies), and modern series commonly report durable improvements in opening and quality of life over time. Long‑term prospective follow‑up has also been reported for patient‑fitted systems used in current practice.1,2,5
Potential risks
As with any major facial surgery, there are risks. We review your specific risk profile during consultation, and we use preventive strategies and close follow‑up to reduce complications. Potential risks may include:
- Temporary weakness of facial nerve branches (often improves as swelling resolves)
- Sensory changes (numbness) around the ear, cheek, or jawline
- Infection, bleeding/hematoma, scarring, or wound healing issues
- Heterotopic bone formation (bone forming where it shouldn’t around the prosthesis)
- Persistent pain, bite changes, or the need for revision surgery in a small subset of patients
Systematic reviews suggest that transient facial nerve weakness and sensory changes are among the more commonly reported complications, while infection and heterotopic bone are less common but important considerations.3,2
3D Virtual Surgical Planning (VSP)
For both TMJ replacement and corrective jaw surgery (when indicated), we often use 3D Virtual Surgical Planning (VSP) — a computerized planning process that combines CBCT (3D CT) imaging with digital bite records (and MRI findings when relevant) to simulate the surgery before you ever enter the operating room. VSP helps us plan jaw position, design patient‑specific components and guides when appropriate, and translate the plan more accurately during surgery.2,4
In select cases, joint replacement can be coordinated with orthognathic (corrective jaw) surgery when jaw position correction is also indicated.
- Lima FGGP, et al. Survival of temporomandibular total joint replacement. 2024 (systematic review/meta‑analysis). PubMed
- Almeida LE, et al. Quality of Life Outcomes Following Total TMJ Replacement. 2025 (systematic review). Full text
- Lima FGGP, et al. Complications of total temporomandibular joint replacement. 2023 (systematic review). PubMed
- Shalabi MM, et al. Accuracy of 3D Virtual Surgical Planning. 2024 (review). Full text
- Rajkumar A, et al. Prospective study of long‑term outcomes and… (TMJ Concepts system). 2022 (10+ year follow‑up). Abstract
- Stryker CMF. TMJ Concepts (manufacturer overview and published literature references). View
- U.S. FDA. TMJ Concepts Patient‑Fitted Implant (PMA) — labeling and device information. PDF
TMJ consultation
Phone: (630) 425-2555
Email: Contact@Horizon-OMS.com